Every morning I wake up, look at my stomach, and hope Winston Churchill is rotting in his grave. While that might sound like a reach, my biology is actually keeping a very specific, very bitter receipt. Most people look at the metabolic crisis in the Bangladeshi community of New York City and call it a “lifestyle phenomenon,” a polite way of saying we just make poor dietary choices. But this framework is lazy; it ignores the deep historical and structural forces that shape a body long before it ever reaches a doctor’s office. What the medical system labels as a personal failure is, in reality, the biological residue of a two-century sequence of colonial extraction, reproductive violence, and systemic labor exploitation. The disproportionate rates of diabetes and metabolic syndrome among Bangladeshi Americans are not random; they are a physical record of historical trauma landed in the bodies of people who are then told the problem is simply what they eat.
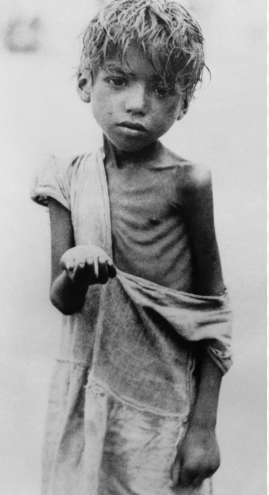
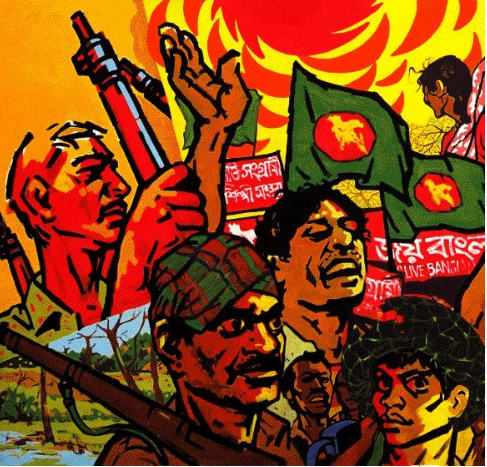
During nearly two centuries of British rule, Bengal’s self-sufficient food systems were dismantled to serve metropolitan markets through cash crop mandates like indigo and jute. This led to 31 famines in just 190 years, a staggering increase from only 17 famines in the preceding two millennia. This cycle of extraction continued into the 1971 genocide, where a campaign of reproductive violence and state-sponsored famine targeted the biological continuity of the Bengali nation through the bodies of women. Emerging research indicates that such severe maternal trauma and acute nutritional deprivation leave an “epigenetic signature” on offspring. These changes to DNA methylation patterns alter stress responses and hormonal regulation, creating a heightened metabolic vulnerability that persists across generations. For the grandchildren of survivors, the risk of disease is not just about today’s diet, but about the starvation and violence our ancestors endured decades ago.
In New York City, this biological vulnerability meets a modern food system built on a similarly extractive logic. While the male street vendor at the halal cart is the visible face of this labor, a largely invisible “female architecture” sustains the entire community. In the Bronx, 74% of Bangladeshi women are overweight or obese by South Asian standards, with staggering rates of diabetes and hypertension. These women often carry a “triple burden”: the formal labor of healthcare where they work grueling 24-hour shifts as home health aides, the informal community food preparation that feeds the city’s workforce, and the unpaid domestic management of the household. Working a 24-hour shift on poverty wages in a body that already carries the biological imprint of generational deprivation is the kind of compounded physical stress that manifests as chronic disease.
The tragedy of this crisis is compounded by a medical system that measures our bodies against the wrong standard. Western BMI cutoffs were designed for European populations, yet South Asians face metabolic risk at much lower thresholds, overweight at 23 rather than 25, and obese at 27.5 rather than 30. By relying on dietary counseling and generic metrics, the public health framework effectively undercounts the risk and ignores the chronic physical stress of 12-hour vendor shifts and 24-hour care shifts. To see this “biological shadow” is to acknowledge that a sociology of food cannot just be about taste; it must account for the colonial histories embedded in the bodies doing the cooking and the women sustaining them at home.




Leave a Reply
You must be logged in to post a comment.